Ovarian Cysts
What is a cyst?
In brief cyst is the general name given to tiny sacs filled with fluid. They are separated from the tissue they form on by a layer called “cyst wall”. They can be, simply, classified into two; benign (dysfunctional) and cancerous (neoplastic) cysts. Most women may encounter cysts in their ovaries in some part of their lives. Cysts in the ovaries do not usually show any symptoms but are recognized during routine gynaecological examination. Ovaries house a variety of different cells in their system due to their embryologic origins. That’s why they are different than all other organs of the body. Another important feature of the ovaries is the fact that they are responsive to hormonal effects. Depending on different hormones, ovaries may become larger or turn into forming cysts.
How do cysts form?
No cell in our body is permanent. While some cells die, others are produced. And all cells produce a variety and amount of fluids. When this fluid, produced in the cells, is more than the amount absorbed, an accumulation of this fluid occurs between the tissues. This abnormal accumulation of excess fluid between tissues is called “oedema/oedema”. These form as swellings in different parts of the body.
If this fluid is covered by a thin layer of tissue, turns into a sac and when the fluid inside is isolated from the outside effects, a lesion forms which, then, is called a “cyst”. They can form on almost all organs in the body (brain cysts, lung cysts, liver cysts etc.) However, almost all cysts in different organs show symptoms easily and at an early stage except for the ovarian cysts. The reason for this is the fact that the cysts in other organs damage the functioning of those. Some ovarian cysts show symptoms by affecting the function of the ovaries while others (mostly) neither affect any functions nor show any symptoms for a long time. What are the symptoms of ovarian cysts? Ovarian cysts can be roughly categorized into two categories; malignant and benign. The most common ones are benign. The most common symptoms of ovarian cysts;
- Irregular menstruation (the most common symptom),
- Abdominal bloating,
- Abdominal or groin pain,
- Digestive system complaints (constipation, painful defecation),
- Urinary tract complaints (frequent need to urinate).
Because these symptoms can be experienced due to many other reasons (not just specific to ovarian cysts), people with such complaints do not suspect ovarian cysts and do not bother too much regarding such complaints.
An ovarian cyst that doesn’t grow too much, can, easily, find some space inside the abdominal cavity and thus, will not cause any bloating or swelling.
Pain is not common regarding ovarian cysts. If there is pain it might mean that the cyst body has grown, has infection or that there might be a problem regarding endometriosis.
On rare occasions, cysts in the ovaries rotate (torsion) or they may rupture, which may lead to severe/acute abdominal pain. In some instances with severe pain, an urgent surgical operation may be necessary. Cysts may press on the uterus causing a frequent need to urinate or press on the rectum, the last part of the bowels causing constipation or painful defecation complaints. Sometimes there might be digestive system complaints such as appetite and weight loss or mild sickness. It should be noted that there are many different types of ovarian cysts and their symptoms or complaints, therefore, might vary as well.
How are ovarian cysts diagnosed?
Ovarian cysts are usually noticed during routine examinations or during a gynaecologic examination due to a different reason and via gynaecologic ultrasound scans.
Important points in evaluating whether cysts are benign or not:
- The age of the patient, (at advanced ages or after menopause: malignant)
- The size and shape of the cyst, (large and irregular shape: malignant)
- Structurally simple or solid (hard on the inside); (if it’s a complex cyst: malignant, if simple, benign)
- Attachment to the surrounding (if strongly attached: malignant)
- Sensitivity.
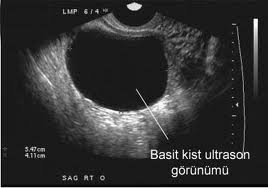
On a pelvic ultrasound scan, cysts smaller than 5-6 cm in diameter and seemingly pure are most probably benign and functional cysts.
However, ones which show papillomatosis (surface elevation), and which are in solid state and bigger than 5-6 cm in diameter, and those causing accumulation of fluid in the abdomen, that are immobile, and those causing hydronephrosis (enlargement of the urinary tract) due to pressure on the kidneys are most probably malignant.
Additionally, cysts that form after menopause (postmenopausal period) are potentially malignant.
Depending on the patient’s and the cysts condition during the first diagnosis, sometimes, computerized tomography (CT) , magnetic resonance imaging (MRI), hormone tests and tumour markers in blood tests may be evaluated to decide on the course of the treatment.
What are tumour markers?
In order to track the condition and development of ovarian cysts tumour markers observed in blood are important. The most common tumour markers are Ca 125, Ca15-3, and Ca 19.9.
BENIGN OVARIAN CYSTS
Benign ovarian cysts are those that do not tend to cause cancer but they may lead to various issues on different levels. Usually, many benign cysts which disappear in time cause unnecessary anxiety. Follicular cysts usually do not reveal any symptoms. Rupture, torsion or acute abdominal pains are hardly the case. Sometimes they can cause irregular menstruation due to oestrogen secretion. The causes of follicular cysts are fully known. Most of the time, they are noticed during an ultrasound examination due to a different reason and the most common symptom is latent menstruation. Follicular cysts usually disappear by themselves and do not require any treatment. Women in their productive ages are observed closely if there are cysts smaller than 5cm. A month later, the patient is called for examination and depending on the situation the cyst is expected to disappear after 1-2 menstruation periods.
Sometimes birth control pills can be given to the patients to help the size decrement of the cysts. The aim is to suppress gonadotropin release in the brain so as to reduce stimulation over the ovaries. A surgical operation may be required when cysts do not become smaller or grow even more despite the treatment. Because such cysts are seen in women who are in their productive ages, only the cyst can be extracted from the ovaries by a laparoscopic method without any damage to the ovaries. That’s because ovaries are one of the most important organs for women.
Follicular cysts
They are one of the most common cysts observed in young generations. It is thought that they form as a result of continuous oocyte (egg cell) growth without hatching. They are usually 2-3 cm and seldom above 4 cm. They are quite stretched, composed of one sac and contain a clear fluid. Usually, they do not cause any complications and most of the time they are noticed by chance during ultrasound scans.
Corpus Luteum Cysts
Generally, after each ovulation, where the egg is released changes into a secretory gland which is called “corpus luteum”. The main function of corpus luteum is to provide the production of a hormone called “progesterone” which makes it possible for the gestational matter (embryo) to attach to the uterus until the placenta becomes fully functional. Progesterone stops the womb from discharging the gestational matter (embryo) because the body might react to it as an alien tissue. Because of its colour, corpus luteum is also called “yellow body”. In time, it might become a cyst due to fluid accumulation inside. Generally, these cysts are 3-4 cm in size, but, they may vary from 1-10 cm. Because they secrete hormones, they might cause delay in menstruation. In case of bleeding within the cyst, there might be pain in the groin. Sometimes it might rupture and lead to bleeding inside the abdomen. In such a case, it might often be mistaken for ectopic (external) pregnancy. If there are no complications, corpus luteum cysts do not require treatment and disappear. Sometimes, corpus luteum cysts can form during the first weeks of pregnancy. These are usually smaller than 3-4 cm in diameter.
Endometriomas (Chocolate Cysts)
Chocolate cysts form as a result of the presence of “endometrium”, a thin layer of intrauterine membrane covering , in the ovaries and that becoming a cyst by bleeding every menstruation.Blood accumulating inside the cyst, every menstruation, for along time, clots and melts; thus, forming a fluid like chocolate both in colour and texture. Hence, the name “chocolate cysts”.Chocolate cysts accompany a condition called “”Endometriosis” and are usually clung to the surrounding. The presence of chocolate cysts shows the severity of endometriosis.It may be diagnosed by observing dense granular cyst bodies inside the ovaries via an ultrasound scan. In the ultrasonography scan, endometrium (chocolate cysts) in the form of one septum (wall) or two septa (walls) can be observed.
Women or young girls with chocolate cysts usually apply to the doctor with complaints such as painful menstruation, pain during sexual intercourse (dyspareunia), infertility, and an increased number of menstruations.
In a differential endometrium diagnosis, mucinous cancer is observed among Neoplastic (cancerous) cysts which form in the ovaries. Differential diagnosis of the case can be made by monitoring serum tumour markers and by analysing doppler blood flow velocity and resistance results. Nevertheless, a definitive diagnosis can be made by a pathological examination of some tissue sample taken via an operation. Treatment of endometrioma involves the extraction of cysts via a surgical operation. Usually, laparoscopic methods are used for such operations.
50% of patients who have had the cysts removed get pregnant in the first 6 months without any treatment.
Cysts smaller than 4 cm are watched closely or some medication treatment (Danazol and Gn RH analogues) may be tried.
Inclusion cysts
They are usually encountered during uterine surgery and are dysfunctional. Inclusion cysts are usually microscopic in size. They do not reveal any symptoms and cannot be detected in ultrasound scans.Inclusion cysts, most probably, form due to confinement of a type of cell called “germinal epithelium” inside the ovarian wall tissue during the healing period of the membrane following every ovulation, when the membrane full body structure is damaged. Some scientists argue that in the long term, these tiny cysts might turn malignant and lead to ovarian cancer.
Theca-lutein cysts
They form as a result of excessive hormone secretion. They are almost always two sided and can reach a size up to 20 cm. They are usually observed in patients having received infertility treatment and in molar pregnancy (grape like cell clusters), which is an abnormal condition of pregnancy. The treatment involves bed rest and close follow up. Sometimes surgical treatment may be required.
Pregnancy luteoma
These are solid cysts observed during pregnancy. Sometimes, they can grow up to 20 cm. A quarter of patients may have complaints regarding excess hair growth and hirsutism during pregnancy due to excessive release of male hormones. They recede when the pregnancy ends. However, they should be differentiated from other tumours.Complications regarding benign ovarian cysts They have two important complications:
- Torsion (twist)
- Rupture (breach/burst)
In both cases, sudden and severe abdominal pain is experienced.
Torsion (Twist)
This is the most feared complication of benign ovarian cysts. Torsion is the twisting/turning of the ovary around itself. Because this will lead to a decrease in or stop the blood flow to the area, there might be gangrene (death of tissue) after a while.A clinical symptom of torsion is continuously increasing levels of pain. Sometimes, however, torsion does not fully occur, which, then, reveals itself through a minor pain.After a while, the ovary may get loose of torsion and by “detorsion” it rotates to its original position and the pain might disappear.The frequency of observed torsion, which is mostly observed in “dermoid cysts”, is 3.2 – 16%. The bigger and heavier the cyst, the higher the risk of torsion.
Ovarian torsion requires immediate surgical operation. Torsioned cyst is completely removed via surgical operation.
Rupture (Burst)
While a cyst might rupture (burst) by itself, it might happen because of torsion.
When rupture is sudden, it builds up a shock. If the content of the cyst is fatty or rich in solid tissue as in dermoid cysts, these tissues can cause a dangerous condition called “chemical peritonitis” by irritating the inner tissue of the abdomen wall (peritoneum).If cyst ruptures lead to internal bleeding or if abdominal pain becomes unbearably acute, the patient should be treated immediately via surgical operation. If complaints are mild and if they decrease in a few hours, the patient is monitored closely.